
Jaw pain isn't just a dental problem. Most TMJ cases start somewhere else entirely.
Clicking, locking, jaw pain, headaches, ear fullness, neck tension. These are the hallmarks of TMJ dysfunction. The jaw, the muscles controlling it, and the cervical spine are all part of the same system.
10 minute read
What is TMJ dysfunction and why does it keep getting mismanaged?
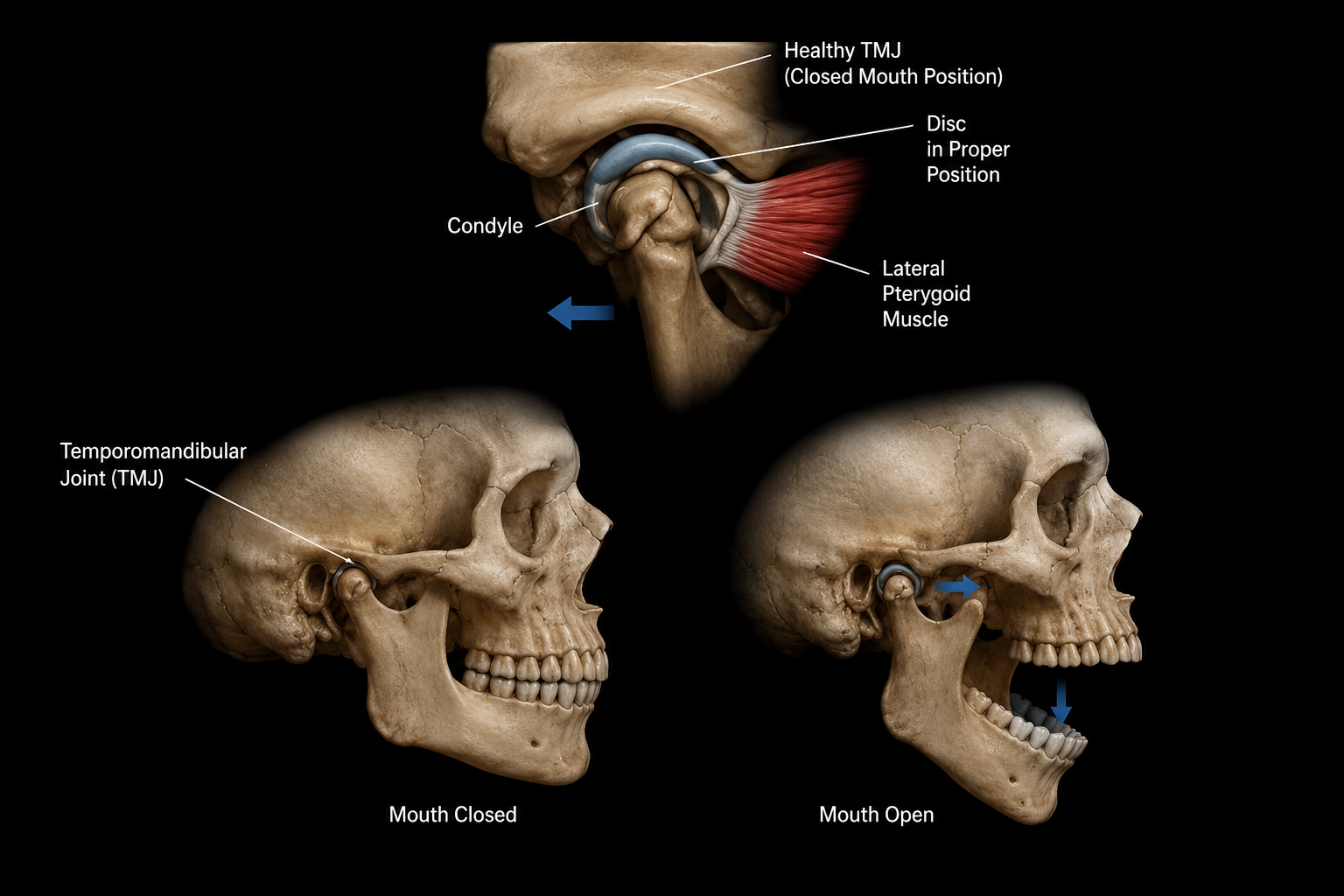
The temporomandibular joint is one of the most complex joints in the body. It's actually two joints, one on each side of the face, that work together to allow the jaw to open, close, slide forward, and move side to side. When either joint, the disc inside it, or the muscles controlling it become compromised, the result is what clinicians call temporomandibular disorder, or TMD.
“25% of adults show signs or symptoms of TMD. Most without a clear diagnosis or effective treatment plan.”
TMD is not a single condition. It's a category covering disc displacement, muscle dysfunction, joint arthritis, capsular tightness, and combinations of all of the above. This is exactly why it gets mismanaged so frequently. "TMJ" gets treated as one thing when it's actually several different problems that each respond to a different approach.
“80.9% average pain reduction in a chiropractic TMD case series. Pain scores dropped from 8.3 to 1.4 on a 10-point scale.”
According to the National Institute of Dental and Craniofacial Research, TMD affects 5 to 12% of the general population. An estimated 25% of adults present with signs or symptoms. And yet most people cycle through dentists, bite guards, and anti-inflammatories without anyone addressing the musculoskeletal drivers that are often at the root of the problem.
What actually causes TMJ dysfunction
-
Inside each TMJ sits an articular disc that cushions the jaw bone against the skull. When this disc shifts out of position — most often forward — it produces the clicking or popping most people associate with TMJ. With reduction means the disc snaps back into place when you open wide. Without reduction means it stays displaced, causing limited mouth opening and jaw locking. Research shows disc displacement is present in 84% of symptomatic TMJ patients compared to 33% of asymptomatic individuals.
-
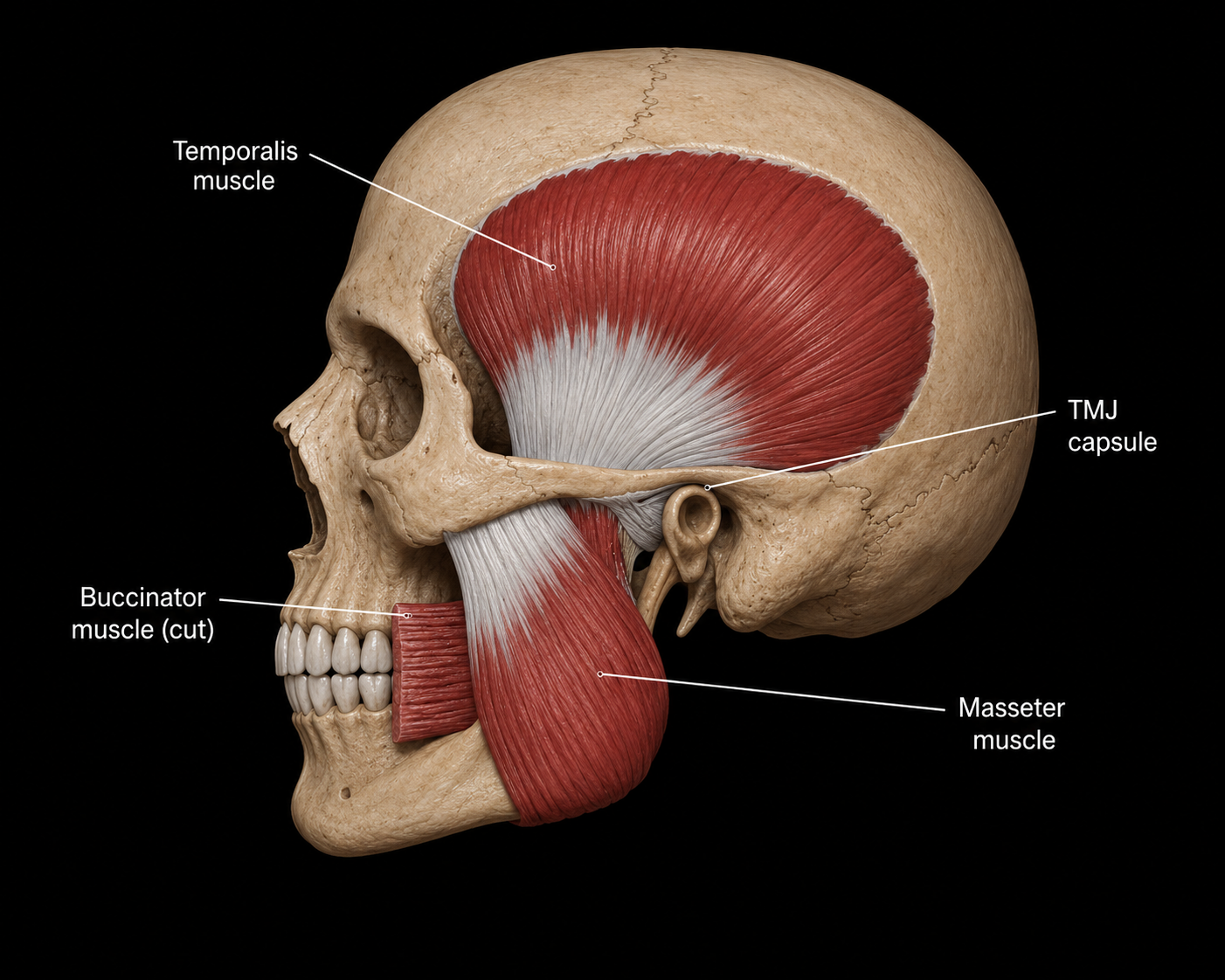
The muscles that power the jaw, including the masseter, temporalis, and pterygoids, are among the strongest muscles in the body relative to their size. When they become chronically overloaded through bruxism, clenching, or sustained stress, they don't just get sore. EMG studies show that TMD patients have measurably elevated bioelectrical activity in the masseter and temporalis muscles both at rest and during function, meaning these muscles are essentially never fully switching off.
That persistent low-grade tension creates a self-reinforcing cycle. Muscle hyperactivity drives joint loading, joint loading drives pain, and pain drives more muscle guarding. Research confirms clenching is present in 60% of TMD patients and bruxism in 30%, both strongly associated with TMJ pain and myalgia. Myalgia is found in 74% of clinical TMD populations.
-
The TMJ and the cervical spine share neurological pathways through the trigeminal nerve. Dysfunction at C2-C3 can produce referred pain in the jaw, face, and ear that is clinically indistinguishable from TMJ arthralgia. Research shows a correlation of r=0.82 between jaw disability and neck disability, a near-perfect relationship. A clinical trial found that treating the neck alone improved TMJ function in patients who never reported jaw symptoms. This connection is one of the most important and most overlooked aspects of TMJ dysfunction.
-
Whiplash, direct jaw trauma, prolonged dental procedures, and chronic forward head posture all alter TMJ mechanics. In sustained cervical flexion, the position most people hold while looking at a phone or laptop, the mandibular condyle is pushed back against retrodiscal tissue, increasing intra-articular pressure over time. Postural correction and cervical rehabilitation are not optional add-ons in these cases. They are part of the primary treatment.
what TMJ dysfunction feels like, including the symptoms most people don't connect to their jaw
TMD produces a wider range of symptoms than most people expect. Many patients don't realize their headaches, ear symptoms, or neck tension are connected to their jaw until a proper assessment makes the link.
Jaw pain or aching, especially in the morning or after eating
Clicking, popping, or grating sounds when opening or closing the mouth
Limited mouth opening or jaw locking
Temple headaches or facial pain
Ear pain, fullness, or ringing (tinnitus) with no ear infection present
Neck pain and upper trapezius tension that persists despite treatment
Tooth sensitivity or pain without a dental cause
Pain or difficulty chewing, or a bite that feels off
Teeth grinding or clenching
The ear symptoms in particular cause significant diagnostic confusion. Because the TMJ sits directly in front of the ear canal and shares nerve pathways with auricular structures, patients frequently present first to an ENT only to find nothing wrong with the ear itself. If you've been told your ears are fine but symptoms persist, TMJ dysfunction is a serious clinical consideration.
The muscles controlling your jaw may be the biggest driver of your pain
This is the section most TMJ treatment skips entirely.
When the masseter and temporalis are chronically overactive, whether from stress, clenching habits, or postural strain, they don't just cause soreness. EMG research shows that TMD patients have significantly elevated muscle activity in these muscles even at rest and during sleep compared to people without TMD. The muscles are running hot all the time.
That sustained hyperactivity does two things. First, it loads the joint continuously, compressing the disc and inflaming the retrodiscal tissue even when you're not chewing or talking. Second, it creates myofascial trigger points. These are dense, hypersensitive nodules within the muscle tissue that refer pain to the temple, the ear, the tooth, and the side of the head. A patient who presents with what appears to be ear pain or tooth pain that has no dental or ENT cause very often has active masseter or temporalis trigger points as the actual pain source.
A randomized controlled trial found that myofascial release applied to the masseter and temporalis produced greater analgesic effects than post-isometric relaxation in female TMD patients, and that soft tissue manual treatment benefits patients with myogenic TMD specifically. A separate study found that deep massage of the masticatory muscles to release trigger points leads to rapid pain relief and improved muscle function, and that deactivating myofascial trigger points should be among the first clinical priorities in TMD treatment.
What this means at NERV: Soft tissue work on the masticatory muscles is not an add-on to TMJ treatment at NERV. It's a primary intervention. Myofascial release and targeted trigger point work applied to the masseter, temporalis, pterygoids, suboccipitals, and suprahyoid group directly reduces the muscle tension that loads the joint, refers pain to the head and ear, and perpetuates the dysfunction cycle.
Treating the neck alone improved TMJ function, even in patients who never had jaw pain
A parallel-group clinical trial studied 60 participants with idiopathic neck pain who had no TMJ complaints. After three weeks of cervical rehabilitation alone, researchers measured significant improvement in TMJ clinical condition without any direct TMJ treatment at all.
The anatomical reason is the trigeminal-cervical complex. The trigeminal nerve and upper cervical spinal nerves converge in the brainstem at the trigeminal nucleus caudalis. Pain signals from the jaw and from the upper neck activate overlapping central pathways, meaning cervical dysfunction genuinely produces jaw pain, and jaw dysfunction genuinely produces neck pain and headaches.
r = 0.82 is the correlation between jaw disability and neck disability across clinical populations. Improvement in one consistently produces improvement in the other.
This is why a comprehensive TMJ assessment at NERV always evaluates the upper cervical spine, head posture, and craniocervical musculature alongside the jaw joint. Treating the TMJ while ignoring a dysfunctional C2-C3 segment or a chronically tight suboccipital group is like treating sciatica without addressing the disc.
What TMJ care at NERV actually looks like
-
We evaluate the TMJ itself, including joint range of motion, disc position, end-feel, and presence of clicking or crepitus, alongside the upper cervical spine, head posture, and masticatory muscle tone. We identify trigger points in the masseter, temporalis, and pterygoids. We look for the relationship between jaw symptoms and neck symptoms rather than treating them as unrelated problems.
-
Myofascial release, targeted trigger point work, and IASTM applied to the masseter, temporalis, pterygoids, suboccipitals, and suprahyoid group. This directly reduces the muscle hyperactivity that loads the joint and refers pain to the head, ear, and teeth. For patients with myogenic TMD, where muscle overactivity is the primary driver, this is often the intervention that produces the fastest and most meaningful relief.
-
When upper cervical dysfunction is identified, including restricted C1-C2 rotation, suboccipital tension, and forward head posture, we address it as part of the TMJ treatment. The research is clear that these structures are connected. Mobilization of the upper cervical spine directly influences TMJ mechanics and symptom patterns.
-
The systematic review evidence is clear. Manual therapy alone produces good short-term TMJ results, but adding therapeutic exercise is what sustains them. We prescribe jaw mobility work, cervical stabilization, and postural correction exercises specific to your presentation. Patients who leave with an activ
FAQs
-
Yes, and the evidence supports it. A retrospective case series published in the Journal of Chiropractic Medicine documented an 80.9% average pain reduction in 14 TMD patients treated with chiropractic care. A systematic review confirmed that manual therapy reduces TMJ pain and improves mouth opening, with sustained results when combined with therapeutic exercise. The key is that effective chiropractic TMJ care addresses the masticatory muscles, the joint mechanics, and the upper cervical spine together rather than the joint in isolation.
-
A bite guard addresses the consequences of grinding. It protects your teeth and may reduce joint loading during sleep. It doesn't address the muscle hyperactivity, trigger points, disc mechanics, or cervical dysfunction driving the problem during waking hours. Most patients with bite guards still have persistent daytime jaw pain, clicking, and headaches because the guard manages symptoms rather than treating the underlying cause. Manual therapy and cervical rehabilitation work on the actual drivers. Both can coexist and often complement each other well.
-
It's neurological and mechanical. The trigeminal nerve and upper cervical spinal nerves converge in the brainstem, meaning pain signals from both regions activate overlapping central pathways. Research shows a correlation of r=0.82 between jaw disability and neck disability. A clinical trial found that treating the neck alone improved TMJ function in patients who had never reported jaw symptoms. Cervical dysfunction is one of the most consistent and most overlooked contributors to TMD.
-
Not necessarily. Clicking without pain is common and often represents disc displacement with reduction, where the disc snaps back into place on opening. Many people have this for years without progression. However, clicking indicates the disc is not tracking normally, and it can progress, particularly when grinding, postural load, or cervical dysfunction are present and unaddressed. Worth having assessed to understand what's driving it and whether any intervention is warranted before symptoms worsen.
-
Yes. Intraoral myofascial release involves working directly on the pterygoid muscles from inside the mouth. The medial and lateral pterygoids are two of the primary muscles controlling jaw movement and position, and they are completely inaccessible from the outside. In many TMD cases, particularly those involving disc displacement, limited mouth opening, or deep jaw aching that doesn't respond to external soft tissue work, the pterygoids are a significant part of the problem. Addressing them directly often produces changes that external treatment alone cannot. It is performed with gloves and is precise. If intraoral work is indicated for your case, we will discuss it with you before proceeding.
Ready to find out what’s actually going on?
Your NERV Origin. 60 minutes.
A real answer. Treatment on day one.
Full assessment, imaging review, and hands-on treatment in a single visit. You leave knowing what’s driving your pain, what the plan is, and already feeling the difference. New patients only.