
A herniated disc
doesn’t need surgery
to get better.
It needs the right system.
Most people with a herniated disc don’t need an operation. What they need is someone who treats the whole picture. At NERV, we combine disc decompression, soft tissue therapy, and movement rehab because the research shows that’s what actually works.
10 minute read
What's actually happening in your spine
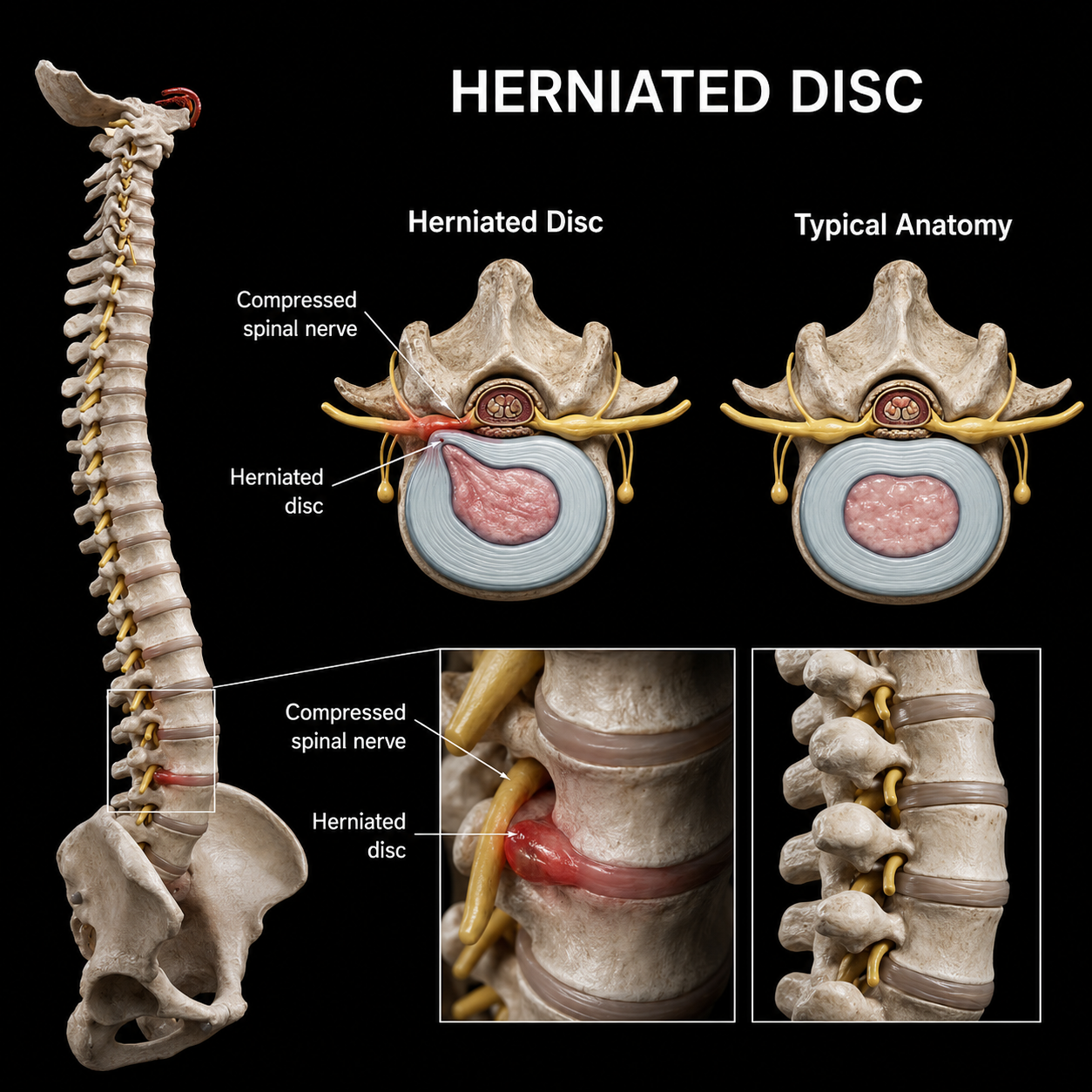
A disc herniation happens when the soft inner material of a spinal disc pushes through a crack in its outer wall, often at L4-L5 or L5-S1 in the lower back, or C5-C6 in the neck. When that material presses against a nearby nerve root, it creates the symptoms most people recognize immediately: shooting pain down the leg or arm, numbness, tingling, weakness, or a burning sensation that seems to have no clear off switch.
What makes disc herniations confusing is that the pain is almost never where the problem is. The disc is in your lower back. The pain is in your calf. The disc is in your neck. The numbness is in your fingers or between your shoulder blades. That disconnect is why so many people spend months treating the wrong place.
The other thing worth knowing: a herniated disc doesn't automatically mean surgery. Most herniations, even large ones, can improve with the right conservative care. The disc itself has some capacity to resorb over time, and the nerve, once the compression is relieved, can recover. The question is whether the treatment you're receiving is actually addressing the right structures in the right way.
By the time most people find us, the disc is only part of the story.
Here's the part most people don't hear about: what a disc herniation turns into after weeks or months of your body trying to manage it. The original injury is one thing. What builds around it, the bracing, the tightening, the compensation patterns your nervous system locks in to protect the area, that's a different problem entirely. And it doesn't go away on its own just because the disc starts to improve.
So now you’re not just dealing with a disc problem. You’re dealing with a disc problem wrapped in a guarding problem, layered with restricted tissue that’s been stiff for months, on top of a movement pattern your body taught itself to avoid pain that now causes its own pain.
That’s why treating one thing at a time doesn’t work.
If we only decompress the disc, the surrounding muscle tension stays. If we only work the soft tissue, the mechanical compression at the disc level is still there. If we only give you exercises, we’re asking your body to build stability on top of structures that haven’t been freed up to move properly yet.
The research backs this up and we’ll show you exactly what it says below. But honestly, it’s just common sense once you see the whole picture. The disc needs to be decompressed. The tissue around it needs to be released. And the muscles that protect the spine need to be retrained to do their job. In that order, together, is how people actually get better.
What the research says about each part of your treatment
-
91% of patients with low back and leg pain got relief with Cox flexion-distraction — averaging 29 days and 12 visits — across a landmark 1,000-case outcomes study.
Most people have never heard of Cox flexion-distraction. Short version: it’s a specialized table that gently stretches and decompresses the spine at the exact disc level that’s causing the problem. No cracking, no twisting, no force applied directly to the injured area. The table moves, the disc gets space, and pressure on the nerve root goes down.
It’s one of the only conservative techniques specifically designed for disc herniation — not just back pain in general. A 2012 clinical study on L4-L5 disc herniation showed statistically significant reduction in disc herniation index after a Cox protocol. A published case in the Journal of Manipulative and Physiological Therapeutics documented a patient with MRI-confirmed disc herniation and nerve compression who completed 10 sessions and was fully pain-free eight months later. No surgery.
Why it matters at NERV
This gets at the disc directly — the actual source of the problem. Everything else we do supports this. Most clinics don’t have the table. We use it as a core treatment, not an occasional add-on.
-
A meta-analysis of 8 randomized controlled trials found myofascial release produced statistically significant improvements in both pain and physical function in chronic low back pain patients.
Think about what happens to your body after months of pain. You’ve been guarding. Your hips are tight. The muscles around your low back have been braced so long they’ve essentially forgotten how to let go. The fascia — the connective tissue that wraps around everything — has started to lock down in compensation patterns that feel like they’re holding you together, but are actually holding you stuck.
This is why some people get decompressed, feel better for a week, and then tighten right back up. The disc responded, but the tissue around it didn’t. Soft tissue work — myofascial release, ART (Active Release Technique), and IASTM — addresses this layer directly. A 2022 systematic review of ART in the Journal of Sport Rehabilitation found it consistently improved patient outcomes across nine peer-reviewed studies. Studies also show combining ART with strengthening exercises outperforms either approach on its own.
Why it matters at NERV
This is the layer most chiropractic offices skip. You can decompress a disc all day — but if the surrounding muscles and fascia are still locked down, the nerve stays under tension. We work through all of it.
-
611 patients across 8 randomized controlled trials — a 2025 meta-analysis confirmed that exercise therapy significantly improves pain, disability, range of motion, and quality of life in lumbar disc herniation.
Here’s the honest truth about disc herniation: decompression gets you out of pain. Exercise keeps you out of pain. Without it, you’re likely to end up back where you started.
When a disc herniates, the deep stabilizing muscles around your spine — the ones that act like a natural brace — often stop firing properly. They don’t turn back on automatically once the pain settles. That’s why so many people feel better for a few months and then re-injure. The 2025 meta-analysis, published in Frontiers in Medicine across 611 patients and 8 clinical trials, found targeted exercise produced meaningful improvements in pain scores, disability ratings, and quality of life — specifically for disc herniation patients, not just general back pain.
A separate landmark trial published in the Annals of Internal Medicine found that combining manipulation with home exercise produced significantly better leg pain outcomes than exercise alone — and patients in the combined group were 1.8 times less likely to need pain medication at 12 weeks.
Why it matters at NERV
The Cox table creates the space. Exercise is what keeps the body from closing it back up. We don’t consider a case finished until you have the tools to manage your own spine.
-
Combined manipulation and home exercise outperformed exercise alone by 10 percentage points on leg pain at 12 weeks — published in the Annals of Internal Medicine, one of the most respected medical journals in the world.
The Bronfort et al. trial randomized 192 patients into two groups: spinal manipulation plus home exercise, or home exercise alone. At 12 weeks, the combined group had significantly less leg pain, less disability, better overall improvement, and higher satisfaction — and were 1.8 times less likely to need pain medication. That gap in medication use grew to 2.6 times at the one-year mark.
And from the broader systematic literature on radiculopathy treatment, the conclusion is consistent: multimodal care — multiple tools working together — outperforms treating just one thing. Every time.
Why it matters at NERV
This is the whole reason our model exists. Not decompression alone. Not soft tissue alone. Not exercise alone. The three together, sequenced for your case, is what the evidence points toward — and what we’ve built our practice around.
What your treatment actually looks like
-
Figure out what’s actually going on first
Full orthopedic and neurological assessment — testing reflexes, strength, nerve tension, and movement patterns — to identify which disc level is involved, and whether it’s purely a disc issue or a combination. We review your imaging. We ask about what you’ve already tried. We don’t skip this step.
-
release the tissue holding the problem in place
ART, IASTM, and myofascial release — targeted at the specific muscles and fascial layers that showed up in your assessment as contributing to the compression. Not a general massage. Specific work on the structures keeping tension on the nerve even after the disc starts to improve.
-
Decompress the disc with the Cox table
Applied at the specific level identified in your assessment. We’re watching your symptoms as we work — looking for centralization (when radiating leg pain starts pulling back toward your spine, meaning the disc is responding). The treatment adjusts each session based on how your body responds.
-
Teach your spine to hold its own
Progressive movement and stabilization work introduced as the acute phase settles. Building the deep stability that keeps the disc from re-herniating under normal stress. You leave each visit knowing what to do — and what to avoid — between sessions. The goal is that you graduate with a body that can manage itself.
How most herniated disc cases progress
Recovery isn’t a straight line but it follows a recognizable pattern when the right structure is in place. Here’s the general arc for most cases we see.
-
Full assessment, imaging review, and first treatment all in the same visit. Most patients notice something shift within the first session — even if it’s subtle. You leave knowing what’s driving your pain, what the plan is, and roughly how long it should take. No vague timelines, no pressure.
-
We typically see acute cases two to three times a week early on so each session builds on the last. The main signal we’re watching for is centralization, which is when that radiating leg pain starts pulling back up toward your spine. That’s your disc responding. Soft tissue work starts in parallel, addressing the guarding pattern that built up around the injury.
-
As the acute symptoms settle, the focus shifts. Less passive treatment, more rehab. We start loading the spine progressively — building the stability that keeps the disc from re-herniating under normal daily stress. Visit frequency drops. You’re doing more of the work between sessions.
-
Most cases reach their ceiling of improvement within 8 to 12 visits. Some complex or long-standing cases need more. We’ll be straight with you throughout about how you’re progressing and if we ever feel your case needs a different kind of help, we’ll say so and point you in the right direction rather than keep you coming in.
FAQs
-
For the vast majority of disc herniations, conservative care should come first. A landmark randomized trial in JMPT found that 60% of sciatica patients — people who had already failed three months of conventional treatment including drugs, PT, massage, and acupuncture — got outcomes from spinal manipulation equivalent to surgical microdiskectomy. The 40% who didn’t respond then went on to surgery and did just as well as the surgery-first group. No harm from trying conservative care first. Surgery has its place — severe neurological deficits, loss of bladder or bowel control — but for most people with a disc herniation and nerve pain, conservative care is the evidence-based first step.
-
Less than most people expect. Herniation size on MRI is a notoriously poor predictor of symptoms and treatment response. Some of the most painful presentations involve relatively small herniations in tight spaces. Large herniations — even extrusions — can and do resorb with conservative care over time. What matters more is whether there’s progressive motor weakness, how the symptoms behave with specific movements, and whether centralization happens early in treatment. We’ll give you a straight clinical read on your case after the assessment.
-
A standard adjustment applies a quick, precise thrust to move a spinal joint — useful for a lot of conditions, but not ideal for disc herniation because it typically involves rotation and compression at the affected segment. Those are the exact movements that aggravate a disc. Cox flexion-distraction works completely differently. A specialized table slowly flexes and distracts the spine at the involved level, reducing pressure inside the disc and creating room for the nerve root — without any rotation or high-velocity force at the painful area. It’s one of the only manual techniques with a research base specifically for disc herniation, not just back pain in general.
-
The table treats the disc. But it doesn’t treat the months of muscle guarding that built up around it, or the deep stabilizers that stopped firing when the injury happened. Those two things — if left unaddressed — will either pull the spine back into the position that caused the problem or leave you without the support structure to stay out of it. The Bronfort et al. Annals of Internal Medicine trial showed that combining manipulation with home exercise produced significantly better outcomes than exercise alone, including 1.8 times lower odds of needing pain medication at 12 weeks. The evidence points clearly toward doing all of it together. That’s what we do.
-
That’s actually the most common thing we hear. When prior treatment hasn’t resolved a disc case, it usually comes down to one of a few things: the technique used wasn’t appropriate for disc pathology specifically, the soft tissue layer was skipped, there was no structured rehab component, or the assessment wasn’t thorough enough to identify what was actually driving the pain. We’ll go through exactly what you’ve had done before we commit to a plan. If we think we can genuinely help, we’ll tell you why. If we don’t, we’ll tell you that too.
Ready to find out what’s actually going on?
Your NERV Origin. 60 minutes.
A real answer. Treatment on day one.
Full assessment, imaging review, and hands-on treatment in a single visit. You leave knowing what’s driving your pain, what the plan is, and already feeling the difference. New patients only.